shoulder Injuries
Rotator Cuff Tears:
Rotator cuff tears are injury or tear of one or more tendons composing the rotator cuff in the shoulder, mainly the supraspinatus, infraspinatus, teres minor, and subscapularis. They serve as tendons connecting the shoulder muscles to the humerus (upper arm bone) and provide stability and movement.
A tear can be partial (where the tendon is frayed or injured) or full-thickness (total detachment from bone). Such injury is usually due to cumulative wear and tear or acute trauma. Individuals with rotator cuff tears usually have shoulder pain, weakness, and trouble with overhead activities like lifting, throwing, or reaching. In advanced cases, it can result in a complete loss of shoulder function and muscle wasting if left untreated.

Causes of Rotator Cuff tears:
- Age-related wear and tear – Over time, tendons naturally lose strength and elasticity, making them more prone to injury.
- Repetitive overhead activity – Sports like tennis, cricket, baseball, or swimming and professions involving lifting or reaching repeatedly strain the rotator cuff.
- Trauma or sudden injury – A fall on an outstretched hand, a heavy lift, or an accident can cause an acute tear.
- Bone spurs – Small bony growths can rub against the tendons, gradually wearing them down.
- Weakness or poor flexibility – When the supporting muscles of the shoulder and back are weak, the rotator cuff tends to absorb excessive stress.
- Age-related wear and tear – Over time, tendons naturally lose strength and elasticity, making them more prone to injury.
Prevention of Rotator Cuff tears:
- Regular strengthening – Exercises that target the rotator cuff and shoulder blade muscles enhance stability.
- Flexibility training – Gentle stretching keeps the shoulder moving smoothly.
- Avoid overuse – Modifying sports techniques or work activities reduces repetitive strain.
- Correct posture and form – Using proper technique in lifting, exercising, and sports protects the tendons.
- Bone and joint health – Adequate calcium, vitamin D, and general fitness help maintain tendon and bone integrity.
- Early medical attention – Seeking treatment for pain or minor injuries prevents small problems from becoming major tears.
Recurrent Shoulder Dislocations:
A shoulder dislocation occurs when the ball of the upper arm bone slips out of its socket. If this happens repeatedly, it is called recurrent dislocation. Patients often describe feelings of instability, fear of certain movements, and pain after the shoulder “slips out.”
This problem is common among young athletes and individuals involved in activities with frequent overhead or contact movements. The more often the shoulder dislocates, the weaker and looser the supporting tissues become, making future dislocations more likely. Treatment usually begins with physiotherapy, but in severe or repeated cases, minimally invasive surgery is often required to restore stability.

Causes of Recurrent Shoulder Dislocations:
- Previous injury – The first dislocation often overstretches or tears ligaments and the labrum, leaving the joint unstable.
- Labrum and ligament damage – A torn labrum (the cartilage rim around the socket) or weak ligaments fail to hold the joint securely.
- Repetitive overhead movements – Swimming, volleyball, and throwing sports can strain the joint.
- Congenital looseness (laxity) – Some people are born with naturally flexible joints, making dislocations more likely.
- High-impact trauma – Falls, sports collisions, or accidents can re-injure an unstable shoulder.
Prevention of Recurrent Shoulder Dislocations:
- Muscle strengthening – Building the rotator cuff and shoulder blade muscles helps stabilize the joint.
- Structured physiotherapy – Guided rehabilitation retrains the muscles and restores shoulder control.
- Avoid risky arm positions – Activities where the arm is pulled back or raised overhead should be limited.
- Safe sports techniques – Learning how to fall safely or play with proper form reduces risk.
- Surgical stabilization – For frequent dislocations, keyhole surgery is highly effective for long-term results.
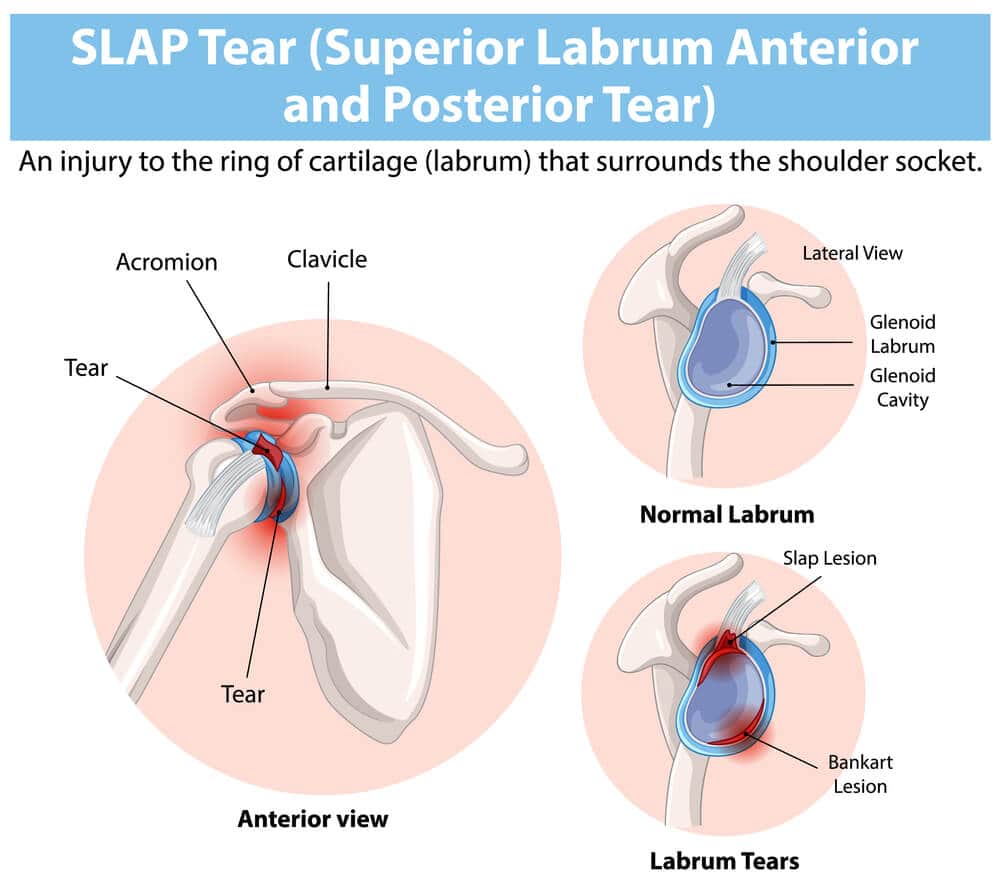
Biceps and SLAP Injuries:-
The biceps tendon attaches the biceps muscle to the shoulder, and the superior labrum (SLAP) is a ring of cartilage that surrounds the shoulder socket. Together, they play a critical role in keeping the joint stable and strong. Injuries to this region—known as SLAP tears or biceps tendon injuries—can cause pain, clicking sounds, weakness, and difficulty with overhead movements like throwing, lifting, or swimming.
These injuries are particularly common among athletes who perform repetitive overhead motions, as well as in people who suffer sudden trauma. Treatment may include physiotherapy, injections, or arthroscopic repair when the damage is significant.
Causes of Biceps & SLAP Injuries:
- Repetitive overhead activity – Sports such as tennis, cricket, baseball, or swimming put repeated stress on the labrum and tendon.
- Sudden trauma – Falling on an outstretched arm, shoulder dislocation, or an accident may tear the tendon or labrum.
- Heavy lifting – Carrying or lifting improperly puts strain on the biceps attachment.
- Degeneration with age – As people age, the tendon and labrum naturally weaken.
- Forceful twisting or pulling – Sudden jerks, such as catching a heavy object, may cause injury.
Prevention of Biceps & SLAP Injuries:
- Balanced muscle strength – Strengthening the rotator cuff, biceps, and shoulder muscles keeps the joint stable.
- Flexibility maintenance – Stretching the shoulder and upper arm reduces the risk of strain.
- Proper technique – Learning correct throwing, swimming, or lifting form prevents overuse injuries.
- Avoid overuse – Incorporating rest days into training gives tendons time to recover.
- Rehab after injury – Physiotherapy following any shoulder trauma reduces the chance of future damage.
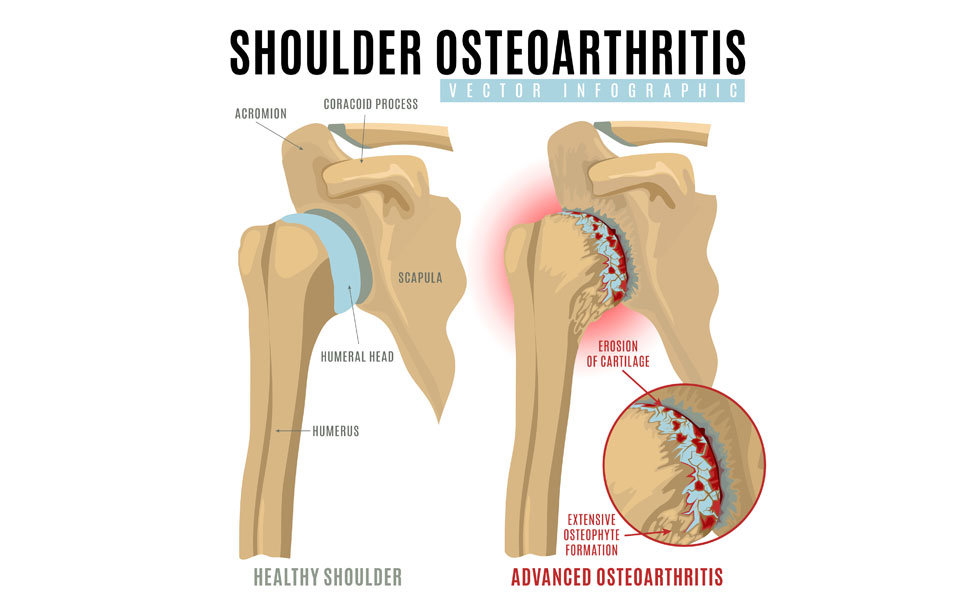
Shoulder Arthritis:-
Shoulder arthritis occurs when the cartilage that cushions the joint surfaces wears away. Without this smooth surface, the bones rub together, leading to stiffness, swelling, and chronic pain. People often notice difficulty with simple tasks like combing hair, lifting objects, or even sleeping comfortably. In the early stages, arthritis can be managed with medications, physiotherapy, and joint injections. In advanced cases where pain and disability are severe, shoulder replacement surgery provides long-term relief and restores function.
Causes of Shoulder Arthritis
- Age-related wear (osteoarthritis) – Cartilage gradually breaks down with age.
- Rheumatoid arthritis – An autoimmune condition that damages joint lining and cartilage.
- Post-traumatic arthritis – Previous injuries such as fractures or dislocations may lead to arthritis years later.
- Rotator cuff arthropathy – Long-standing untreated tears can cause the joint to degenerate.
- Genetic predisposition – Family history increases the likelihood of arthritis.
Prevention of Shoulder Arthritis
- Maintain strong muscles – Regular shoulder and back exercises reduce strain on the joint.
- Protect from injuries – Using proper techniques during sports and daily activities helps prevent damage.
- Avoid repetitive strain – Limiting high-impact or repetitive shoulder tasks prevents overload.
- Keep a healthy weight – Lessens pressure on weight-bearing joints, including the shoulder.
- Treat injuries promptly – Timely care for rotator cuff tears or dislocations can prevent later arthritis.
Treatment Options for Shoulder Conditions
Arthroscopic (Keyhole) Surgery
This minimally invasive procedure uses small incisions and a camera to treat conditions like rotator cuff tears, SLAP injuries, and labral repairs. It offers quicker recovery, less scarring, and faster return to daily activities compared to traditional open surgery.
Minimally Invasive Surgeries
Advances in surgical techniques allow many procedures to be performed with smaller cuts, resulting in less tissue damage, reduced scarring, shorter hospital stays, and faster recovery times.
Shoulder Replacement (Total or Reverse)
- Total Shoulder Replacement – Damaged joint surfaces are replaced with artificial implants, restoring smooth motion.
- Reverse Shoulder Replacement – Designed for patients with irreparable rotator cuff damage, this procedure shifts the mechanics of the joint to allow other muscles to take over shoulder movement.
Regenerative Therapies (PRP / Stem Cell)
Platelet-Rich Plasma (PRP) and stem cell therapies use the body’s natural healing abilities to repair damaged tissues. These treatments are particularly beneficial for tendon injuries, early arthritis, and muscle strains, offering a non-surgical option for pain relief and improved shoulder function.